About Myositis
Myositis is an inflammation of the muscles.
- Myositis abbreviations to know:
- PM: Polymyositis
- DM: Dermatomyositis
- JDM: Juvenile dermatomyositis
- IBMP: Inclusion body myositis
- IMNM: Immune mediated necrotizing myositis
- CADM: Clinically amyopathic dermatomyositis
- ILD: Interstitial lung disease
- Ages of onset:
- DM: Bimodal
5-15 yo, 45-65 yo - PM: 50-60 yo
- IBM: >50 yo
- DM: Bimodal
-
Dermatomyositis > polymyositis can be associated with malignancy
- Symmetrical, proximal muscle weakness= hallmark of inflammatory myositis. If pain >>> weakness: consider alternate etiology (rhabdo, endocrinopathy)
- Classic rash distributions (Gottron’s papules over dorsum knuckles, heliotrope rash, etc.) with muscle weakness should prompt work up for dermatomyositis
- Vast majority of JDM cases have skin involvement
- HyperCKemia doesn’t equate to myositis – different sexes and races can have different “normal limits” also.
- Exercise and dehydration can also impact CK levels.
- Inclusion body myositis is most common myositis of elderly.
- Remember distal and proximal muscle weakness with neuropathic features
- Dermatomyositis and antibodies to NXP and TIF1gamma in adults highly associated with malignancy, but dermatomyositis rarely associated with cancer in children
Proximal muscle WEAKNESS >> pain
Clinical Phenotypes
- PM
- DM: Myositis with rash
- CADM: Typical skin rashes of DM, without weakness
- JDM: Juvenile onset
- IBM:
- Proximal+distal mm
- Asymmetrical
- Inflammation and degeneration
- IMNM:
- Necrotizing myositis
- HMG-CoA reductase antibody in >90%, often with statin use
DM Rashes
- Gottron’s papules (PIPs) (view image)
- Heliotrope rash (around eyes) (view image)
- Shawl sign (view image)
- Photosensitivity
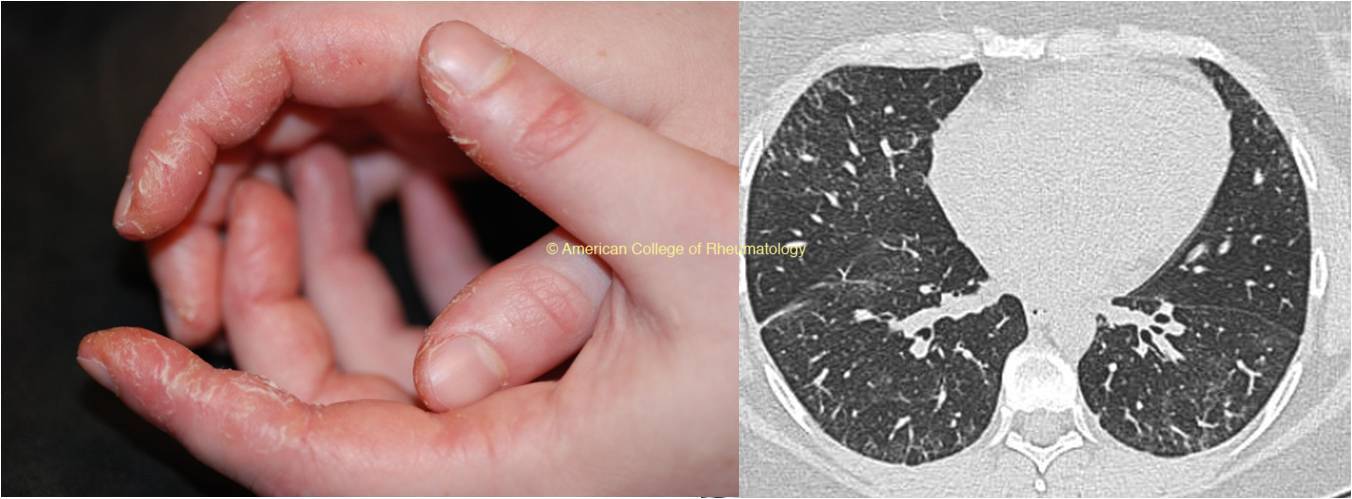
Antisynthetase Syndrome
- Myositis + skin (mechanic hands) + interstitial lung disease (view images)
Other Organs
- Pulm (interstitial lung)
- GI (dysphagia)
- Cardiac (myocarditis)
Lab Workup
- Creatine kinase high
- Aldolase high(some)
- ESR/CRP high
- AST/ALT elevation
- Myglobinuria
- +ANA in a subset
- Myositis-specific antibodies per rheumatologist
Imaging
- Muscle MRI with contrast can show muscle edema of affected muscles
- Chest CT if interstitial lung disease is suspected
- ILD CT protocol = high resolution, prone with deep inspiration
Additional Tests
- EMG shows myopathic changes
- High sensitivity, low specificity
- Muscle biopsy can be diagnostic.
- Swallow study if dysphagia is reported.
Rheumatic
Endocrinologic
- Diabetes
- Hypo/Hyper- thyroidism
Viral Infections
Neuromuscular
- Muscular dystrophies
- Neuromuscular junction disorder
- Denervating disorders
Metabolic myopathy
Rhabdomyolysis
Drug Toxicity
- Glucocorticoids
- Statins
- Colchicine
- Cocaine, Alcohol
Fibromyalgia
Initial Treatment
- Steroids: PO/IV Prednisone equivalent to 1-2 mg/kg/day, then slow taper over months
- IVIg
Long-term Immunosuppression per Rheumatology
- Mycophenolate
- Methotrexate
- Azathioprine
- Tacrolimus
- Rituximab
- Abatacept
PT
Physical therapy and rehabilitation are very important to continue long-term.
Monitoring
- Labs to follow:
- CK/aldolase
- CRP
- Muscle strength
- Monitor for signs of lung siease
- Follow up with PFTs + lung imaging
- Screen for underlying malignancy with age appropriate screening and SPEP/UPEP (esp for dertmatomyositis)
Prognosis
- IBM and IMNM tend to have more difficult response to treatment