About Systemic Sclerosis
Systemic sclerosis (SSc) is a systemic autoimmune disease with characteristic interstitial, vascular fibrosis in the skin +/- internal organs.
Differential Diagnosis
- If there is no Raynaud’s and/or ANA is negative, SSc is rarely the diagnosis!
- Scleroderma renal crisis (SRC): usually with diffuse SSc and early on in disease (first 5 yrs) – presents with sudden increase of BP
- Labs: creatinine increase, MAHA
- ACEi rx
Treatment & Monitoring
- Avoid high dose glucocorticoids due to risk of renal crisis: steroids do not decrease skin tightening
- Interstitial lung disease (ILD) carries high mortality and seen more with anti-Scl-70
- Pulmonary HTN is high cause of death for limited SSc
- Close monitoring of BPs and serial TTEs and PFTs are key
Key Subtypes
Limited SSc (lSSc)
- Skin tightening distal to elbow/wrist, knee/ankle
- CREST: Calcinosis
- Raynaud’s (>90%) (view image)
- Esophageal reflux
- Sclerodactyly (view image)
- Telangiectasia (view image)
Diffuse SSc (dSSc)
- Skin tightening in proximal extremities and trunk
SSc Sine Scleroderma
- SSc antibodies
- Internal organ involvement
- No skin tightening
Localized Scleroderma (skin limited)
- Morphea
- Linear scleroderma
Evaluation Guide
- Concern for systemic? Extradermal?
- Pattern of skin dz? Diffuse or limited to extremities?
- What internal organs involved?
- Raynaud’s (view image)
- Esophageal
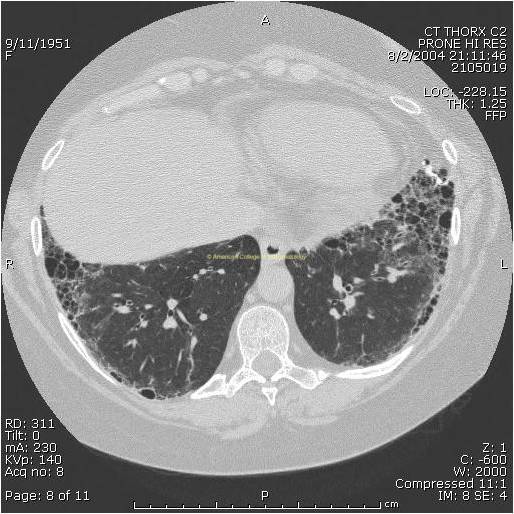
- Lung: ILD: PFTs, high-res CT w/o contrast (view image), chest
- pHTN: DLCO, TTE
- Renal: Scleroderma renal crisis (SRC)
- Heart
- Myositis
Basic Labs
- CBC (anemia of chronic disease, MAHA)
- CMP
- ESR/CRP
- Urinalysis
SSc Serologies
- ANA (80-90%)
- SCL70/topoisomerase: dSSc
- Centromere: lSSc
- RNA polymerase III: SRC
- Scleredema (DM2)
- Scleromyxedema (malignancy?)
- Perineoplastic?
- POEMS
- Chronic graft vs. host disease
- Nephrogenic systemic fibrosis
- Eosinophilic fasciitis
- Amyloidosis
- Drug exposure (e.g., bleomycin)
- Environmental exposure (organic solvents, etc.)
- Highly recommend rheumatology referral before initiating treatment
- Treatment is based on extent of skin disease, organs involved, severity of disease
- Avoid prednisone >=20 mg (associated with scleroderma renal crisis [SRC])
- Skin fibrosis: consider methotrexate (MTX), mycophenolate (MMF)
- Raynaud’s: CCB, PDE5-inhibitor
- Arthritis: hydroxychloroquine (HCQ), MTX
- Interstitial lung disease (ILD): MMF, cyclophosphamide, anti-fibrotics
- Renal crisis: ACEi
- pHTN treatment
- GERD/dysphagia: PPI, reflux rx, GI referral
- Manage BP to decrease risk of renal crisis
- SRC is an emergency!
- Extra-derm disease:
- ILD (view image)
- pHTN
- Renal crisis (20% of dSSc, 5% of lSSc)
- Myopericarditis
- CBC, CMP: monitored for drug toxicity and disease activity
- Follow-up testing for organs of concern: PFTs with DLCO, TTE, CT chest, GI scope
- Cancer screening