About Juvenile Dermatomyositis
Juvenile dermatomyositis (JDM) is an inflammatory, autoimmune disease that primarily affects skin, muscles, and joints.
- Peak age of onset: 7 yo
- Range: 1-15 yo
Clinical Presentation
- Muscle weakness is a prominent symptom, not myalgia
- Vast majority of patients with JDM have skin disease
- Dermatomyositis in children is rarely associated with malignancy
- Bones are often weak due to chronic inflammation and/or steroid therapy
Management
- Sunscreen is important in preventing disease flare.
MSK Exam
- Muscle weakness primarily in proximal limb-girdle, neck, and trunk
Skin
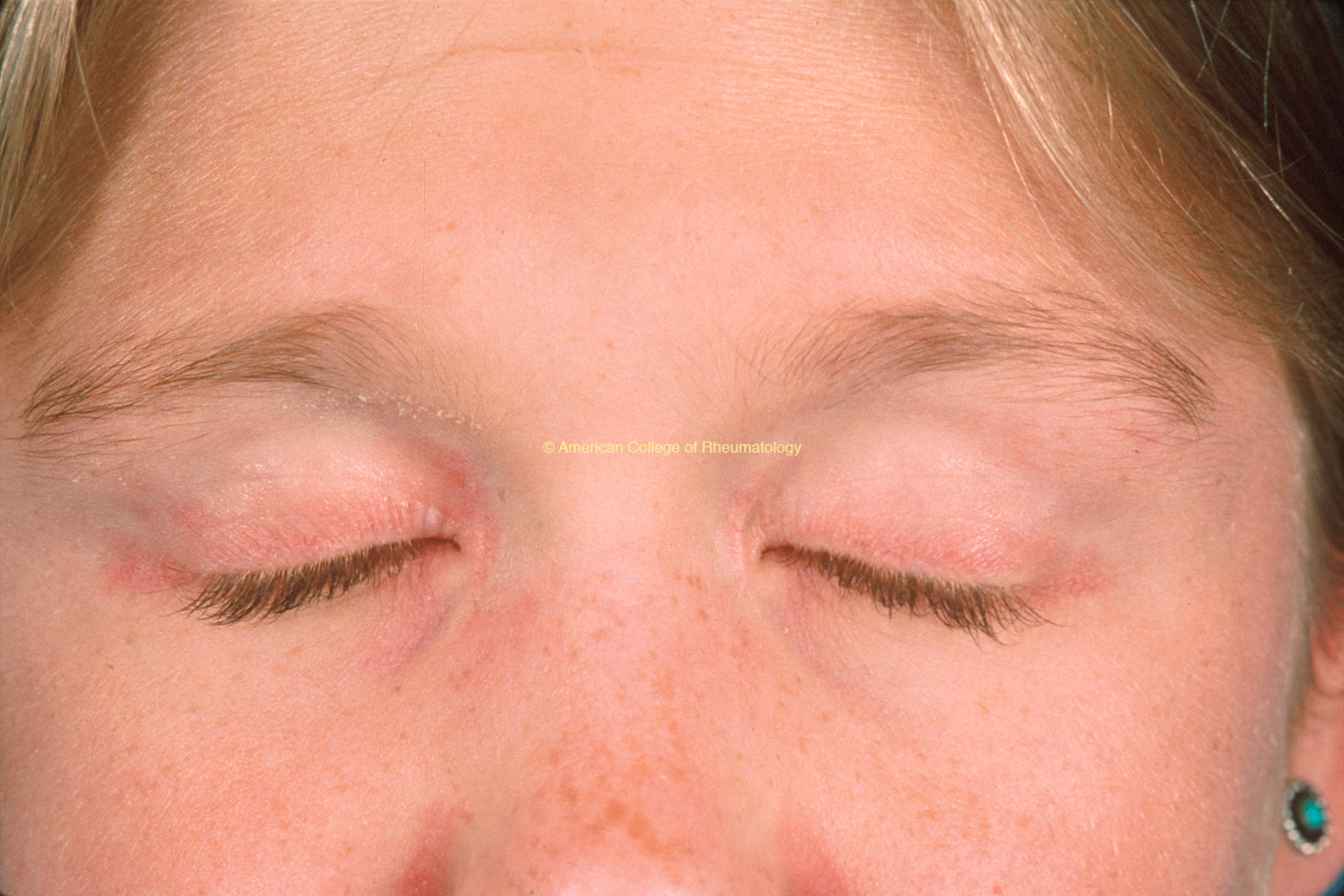
- Heliotrope rash (view image)
- Gottron’s papules (view image)
- Malar rash/facial erythema (view images)
Other Organ Involvement
- Respiratory (interstitial lung disease)
- GI (dysphagia, aspiration, intestinal vasculopathy)
- Cardiac (cardiomyopathy)
Lab Workup
- Muscle enzymes: CK, AST, ALT, LDH, aldolase
- CRP and ESR not markedly elevated
Imaging
- MRI w/o contrast to look for muscle enhancement, muscle atrophy and/or fatty infiltration
- X-rays can show calcinosis in extremities
- Other inflammatory myopathies
- Juvenile polymyositis
- Myositis associated with other connective tissue diseases (e.g. lupus)
- Post-infectious myopathy
- Non-inflammatory myopathy:
- Muscular dystrophy
- Metabolic myopathy
- Thyroid dysfunction
Pharmacologic
- Corticosteroids (wean over time)
- Methotrexate
- IVIG
- Plaquenil (good for skin disease)
Non-Pharmacologic
- Physical therapy
- Occupational therapy
- Suncreen
- Monitor for other organ involvement (cardiac, lung, GI)
- Early treatment to prevent:
- Joint contractures
- Irreversible skin damage
- Appropriate growth of mm and bones
- Risk for osteopenia and pathologic fractures from steroids