About Crystalline Arthropathies
- Gout monosodium urate (MSU) crystal deposition
- M predominance
- Most common inflammatory arthritis for older males
- Peak onset: 40-60yo
- Calcium pyrophosphate deposition disease (CPPD): CPP crystal deposition
- Disease of elderly, onset >50yo
- Likes damaged joints
- F predominance
- Basic calcium phosphate (BCP): BCP crystal deposition
- Predilection for shoulder
Clinical Presentation & Diagnostic Workup
Crystalline Arthritis
- Mimics infection:
- High CRP
- High WBC in joint fluid
Gout
- Almost never diagnosis for premenopausal female
- Podagra: Sufficient for gout dx.
Note: Osteoarthritis (OA) has noninflammatory 1st MTP pain - Gout flare most common risk factors:
- Beer
- Diuretics
- Red meat
- AKI
CPPD
- Can mimic seronegative rheumatoid arthritis
BCP
- Shoulder tendons/bursa most common, AKA “Milwaukee shoulder”
Treatment
- Colchicine:
- Works best when started within first 24-48 hours of flare onset
- Metabolized by CYP3A4- risk of toxicity with CYP3A4 inhibitors (macrolides, antifungals, grapefruit juice)
- After steroid taper for acute treatment, watch for rebound arthritis – slow down taper
- Allopurinol can rarely cause severe cutaneous adverse reactions like SJS
Gout
- Podagra: Inflammatory arthritis in 1st MTP
- Abrupt onset: Severe joint pain & swelling (view image)
- Triggers: Beer, red meat, other alcohol, seafood, high fructose drinks
CPPD
- Chronic: Crystal deposition without flare
- Acute flare: Acute, severe arthritis
- Knee, wrist, 1st & 2nd MCPs
BCP arthritis
- Most common: Acute calcific arthritis and periarthritis of the shoulder (view image)
Arthrocentesis
- Gold standard for diagnosis of crystalline arthropathies
- Synovial fluid analysis: crystals, cell count+diff, Gram stain,culture
Polarized Microscopy
- MSU crystals (view image):
- Needle-shaped
- Negatively birefringent
- CPP crystals:
- Rhomboid shaped
- Positively birefringent
- Alizarin red stain needed to identify BCP crystals
Labs
- Serum uric acid
- CBC CMP
- ESR
- CRP
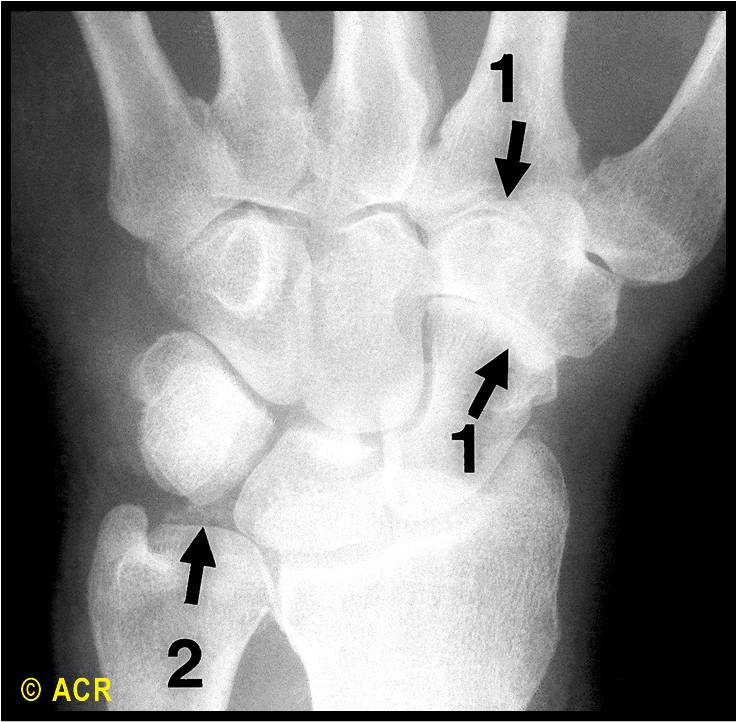
Imaging
- Radiographs
- MSK ultrasound
- Dual energy CT
Septic arthritis
Other Rheumatologic Disease
Endocrinopathy
- Thyroid disease
- Hemochromatosis
Acute Treatment
- NSAIDs
- Colchicine: Acute flare dosing=1.2mg then 60min later, 0.6mg
- Glucocorticoids
- IL-1 inhibitor
- Intra-articular steroids
Long-Term Treatment
Goal: Flare prevention
- Gout
- Dietary and lifestyle modifications: Low purine diet, weight loss, etc.
- Serum uric acid<6 mg/dL
- Urate lowering drugs (allopurinol, febuxostat, probenecid, pegloticase)
- CPPD
Gout
- Target sUA < 6 mg/dL to reduce frequency of flares
CPPD
- Complication includes spinal involvement of C1/C2 joint:
- Called “Crowned Dense Syndrome”
- Can mimic infection
BCP Arthritis
- Surgical or arthroscopic debridement of large symptomatic or recurrent calcific deposits may be necessary